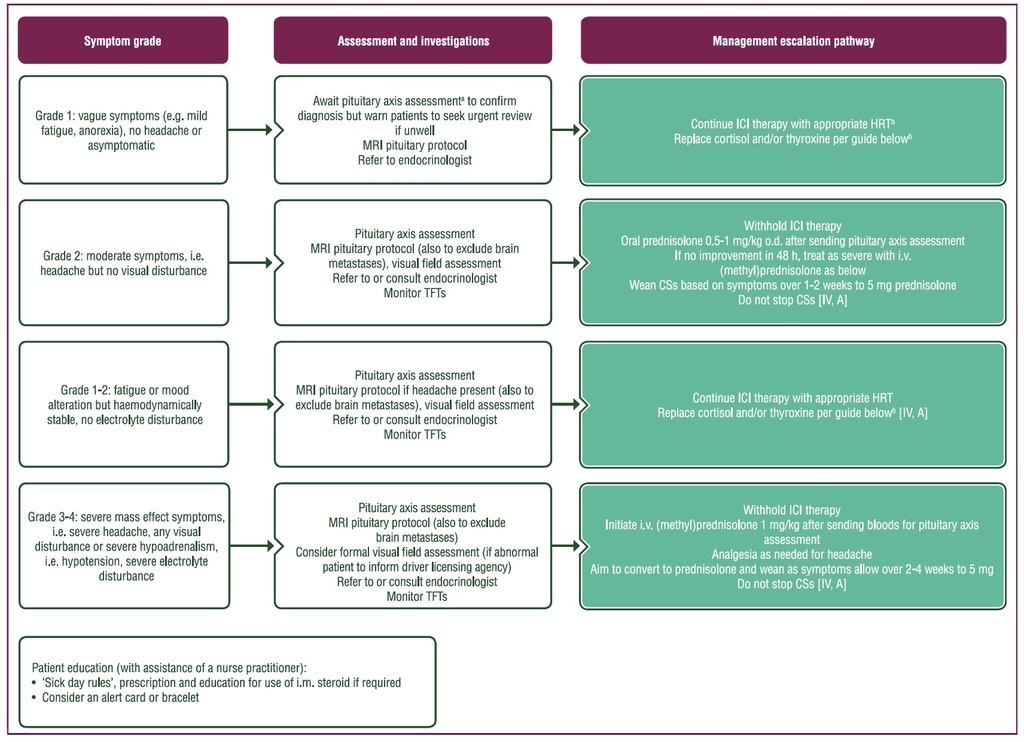
Purple: general categories or stratification; turquoise: combination of treatments or other systemic treatments; white: other aspects of management.
ACTH, adrenocorticotropic hormone; CS, corticosteroid; FSH, follicle-stimulating hormone; FT4, free thyroxine; HRT, hormone replacement therapy; ICI, immune
checkpoint inhibitor; IGF-1, insulin-like growth factor-1; i.m., intramuscular; IR, immune-related; i.v. intravenous; LH, luteinizing hormone; MRI, magnetic resonance
imaging; o.d., once a day; T4, thyroxine; TSH, thyroid-stimulating hormone; TFT, thyroid function test.
Pituitary axis bloods: 9 am cortisol (or random if unwell and treatment cannot be delayed), ACTH, TSH or FT4, LH, FSH, estradiol if premenopausal, testosterone in men,
IGF-1, prolactin. Mineralocorticoids replacement is rarely necessary in hypopituitarism.
bInitial replacement advice for cortisol and thyroid hormones:
Source:
Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up
Published online: 18 October 2022
J. Haanen, M. Obeid, L. Spain et al, on behalf of the ESMO Guidelines Committee
It is a long established fact that a reader will be distracted by the readable content of a page when looking at its layout